Cardiac Cycle
Definition
It is the cardiac events that occur from the beginning of one heart beat to the beginning of the next coordinated by the conducting system of the heart.
Consists of alternating contraction and relaxation of the myocardium
Cardiac Events
Cardica events during one cycle
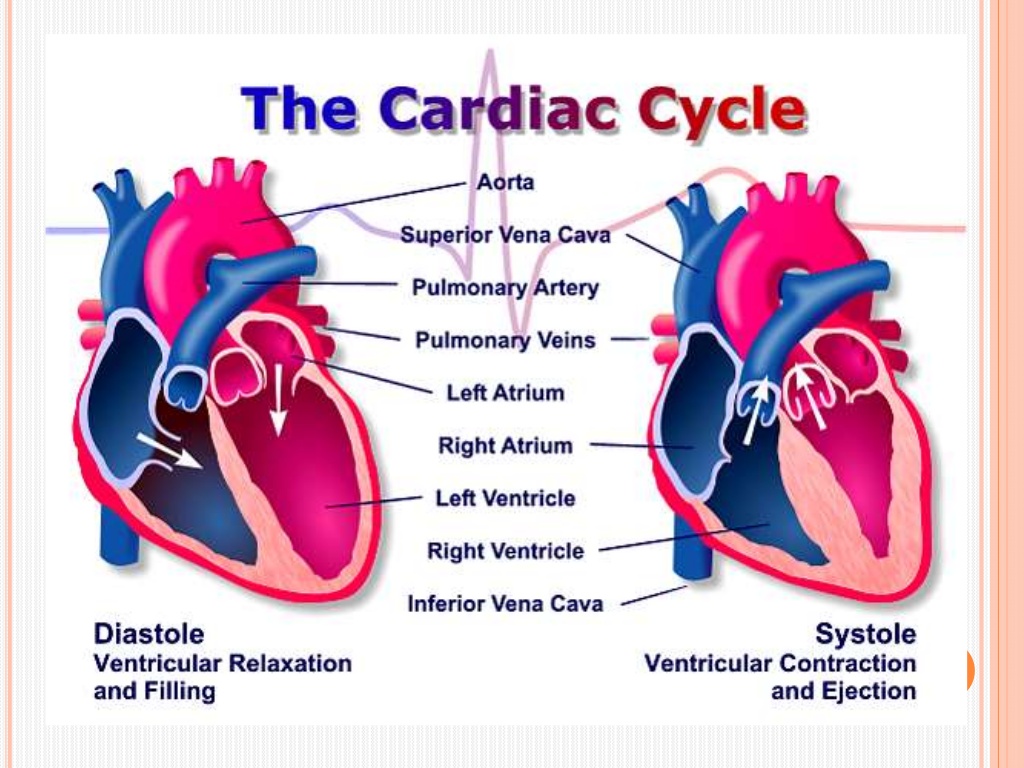
The cycle is divided into two major phases
Systole :- The period of ventricular contraction -
Diastole :- The period of ventricular relaxation
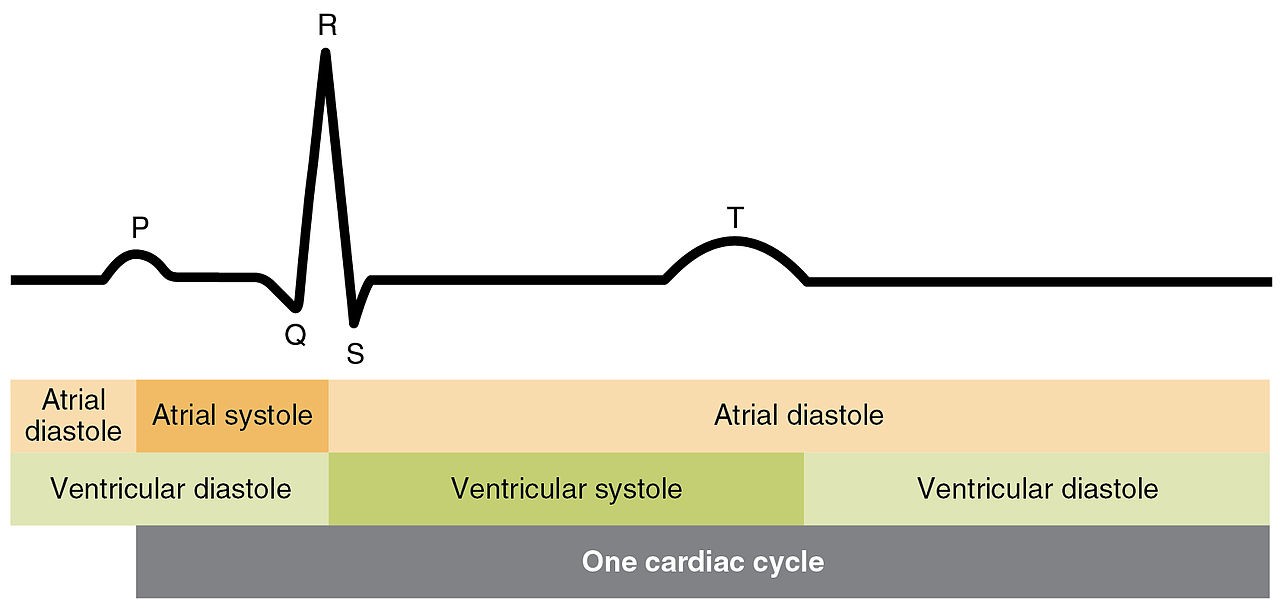
The cycle is futher subdivided into several discrete phases :-
The phases and the duration are as follows:-
Total ventricular systole 0.3 sec
Isovolumic contraction 0.05 sec (0.015sec for RV)
Maximal ejection 0.1 sec
Reduced ejection 0.15 sec
Total ventricular diastole 0.5 sec
Isovolumic relaxation 0.1 sec
Rapid filling phase 0.1 sec
Slow filling 0.2 sec
Atrial systole 0.1 sec
GRAND TOTAL (Syst+Diast) = 0.8 sec
1 Beat = 0.8 sec (800 msec)
Systole = 0.3 sec
Diastole = 0.5 sec
Heart Sounds
S1
Due to closure and after vibrations of AV Valves.
S1 is normally split (~0.04 sec) because mitral valve closure precedes tricuspid closure. (Heard in only 40% of normal individuals)
S1 heart sound
low pitch and relatively long-lasting
S1 is a relatively prolonged, low frequency sound, best heard at apex
S2
S2 is heard when the semilunar vlaves close.
A2 is heard prior to P2 as Aortic valve closes prior to pulmonary valve (A2 aortic valve sound P2 pulmonary valve sound)
Normal split: Two components heard during inspiration and is single sound during expiration.
Common causes of wide split S2
RBBB
Sev PAH
ASD
Idiopathic dilatation of pul artery
Sev right heart failure
Moderate to severe PS
Severe MR
Causes of reverse split S2
LBBB
RV pacing
RV ectopy
Severe AS
Acute MI
WPW type B
Severe TR
Aneurysm of ascending aorta
Severe systemic hypertension
S3
Causes of S3
Physiological: Childrens & young adults <40 yrs (nearly 25%)
(Not heard in normal infants & adult >40 yrs.)
Pathological:
Ventricular failure
Hyperkinetic state (anemia, thyrotoxicosis, beri-beri)
MR, TR
AR, PR
Systemic AV fistula
S4
S4 (atrial or presystolic gallop) - atrial emptying after forcible atrial contraction. (late diastolic)
Caused by vibration of ventricular wall during rapid atrium emptying into non compliant ventricle
Causes of S4
Physiological;
>60yrs (Recordable, not audible)
Pathological;
All causes of concentric LV/RV hypertrophy
Coronary artery disease
Acute regurgitant lesions
An easily audible S4 at any age is generally abnormal.
In contrast to S3, which may mean ventricular failure, the presence of S4 does not indicates heart failure. It only signify "hardworking ventricle".
Gallop rhythm
A gallop rhythm is a grouping of three heart sounds that together sound like hoofs of a galloping horse.
For more on heart sounds scroll down . . . .
* * * * * * * * * * *
Atrial Systole
Heart Sounds
S4 (atrial or presystolic gallop) - atrial emptying after forcible atrial contraction.
appears at 0.04 s after the P wave (late diastolic)
lasts 0.04-0.10 s
Caused by vibration of ventricular wall during rapid atrium emptying into non compliant ventricle
Causes of S4
Physiological;
>60yrs (Recordable, not audible)
Pathological;
All causes of concentric LV/RV hypertrophy
Coronary artery disease
Acute regurgitant lesions
An easily audible S4 at any age is generally abnormal.
Clinical Facts about S4
In contrast to S3, which may mean ventricular failure, the presence of S4 does not indicates heart failure. It only signify "hardworking ventricle".
The presence of S4 correlate with a gradient of at least 50mmHg across LVOT in suspected LVOT obstruction.
(This correlation is not applicable in HCM)
In setting of MI, an audible S4 indicates that at least 10% of myocardium is at jeopardy.
In presence of Shock, S4 indicates that hypovolemia is unlikely as PCWP will be >18mmHg.
S4 can be heard when RVEDP >12mmHg on Rt or LVEDP > 15mmHg on Lt side. If EDP is very high i.e. >25 mmHg, S4 may be absent b/c of insufficient atrial functions.
S1 is d/t closure and after vibrations of AV Valves. (M1 occurs with a definite albeit 20 msec delay after the LV-LA pressure crossover.)
S1 is normally split (~0.04 sec) because mitral valve closure precedes tricuspid closure.
(Heard in only 40% of normal individuals)
S1 heart sound
low pitch and relatively long-lasting
Some Clinical facts about S1
S1 is a relatively prolonged, low frequency sound, best heard at apex.
Normally split of S1 (~40%)is heard only at tricuspid area.(As tricuspid component is heard only here.)
If S1 is equal to or higher in intensity than S2 at base, S1 is considered accentuated.
Variable intensity of S1 and jugular venous pulse are highly specific and sensitive in the diagnosis of ventriculoatrial dissociation during VT, and is helpful in distinguishing it from supraventricular tachycardia with aberration.
Heart Sounds : S2 is heard when the semilunar vlaves close.
A2 is heard prior to P2 as Aortic valve closes prior to pulmonary valve
S2 heart sound
Appears in the terminal period of the T wave
lasts 0.08 - 0.12s
Some clinical facts about S2
Normal split: Two components heard during inspiration and is single sound during expiration.
(A2-P2 ~20- 50 msec in inspiration)
Clinically split is defined as wide, if it is heard well in standing position, in expiration (normally not heard as the split is 15 msec, which can not be heard by human ears)
Single S2: absence of audible split in either phase of respiration.
Fixed split: two components fails to move with respiration.
Reverse split: Inaudible split during inspiration and audible split during expiration. (recognized by wider split in expiration)
Common causes of wide split S2
RBBB
Sev PAH
ASD
Idiopathic dilatation of pul artery
Sev right heart failure
Moderate to severe PS
Severe MR
Normal variant
Common causes of wide fixed split S2
ASD
All causes of wide split with associated severe right ventricular failure.
Common causes of single S2
Truncus arteriosus
Pulmonary atresia
Aortic atresia
TGA
AS, PS
Single loud P2 in extreme PAH
Causes of reverse split S2
LBBB
RV pacing
RV ectopy
Severe AS
Acute MI
WPW type B
Severe TR
Aneurysm of ascending aorta
Severe systemic hypertension
Clinical facts about S3
In presence of HF, S3 correlates well with ventricular end diastolic pressure and is usually >25mmHg on left side.
Right sided S3 correlate well with rapid y descend in neck veins.
Normal A2-S3 interval is between 120-160 msec.
Correlates of S3
Gallop rhythm
A gallop rhythm is a grouping of three heart sounds that together sound like hoofs of a galloping horse.
Protodiastolic gallop or ventricular gallop or S3 gallop
addition of an S3 to the physiological S1 and S2 creates a three-sound sequence, S1-S2-S3.
Presystolic gallop rhythm or atrial gallop
addition of an S4 to the physiological S1 and S2 creates a three-sound sequence, S4-S1-S2.
(during tachycardia S4-S1 can fuse, producing a summation gallop )
Causes of S3
Physiological: Childrens & young adults <40 yrs (nearly 25%)
(Not heard in normal infants & adult >40 yrs.)
Pathological:
Ventricular failure
Hyperkinetic state (anemia, thyrotoxicosis, beri-beri)
MR, TR
AR, PR
Systemic AV fistula
1. Define cardiac cycle and mention its duration. Discuss the different phases in cardiac
cycle and add a note on heart sounds. (2+6+2=10)
* * * * * * * * * * *